On July 16th, 2021, Web MD published an article titled, “Large Remdesivir Study Finds No Survival Covid-19 Benefit”. The study was conducted by the VA, which showed no changes in survivability in VA patients that had Covid-19, with and without the use of remdesivir. There are other studies that have the same conclusion going back to 2020. Yet the latest update from the NIH on July 8th, 2021, states that remdesivir is the only drug approved by the FDA for the treatment of Covid-19.
The question is, why doesn’t remdesivir work?
One of the main reasons that it doesn’t work, is that it is given too late in the disease process. By the time a Covid-19 patient meets the criteria for admission to the hospital, there is a decrease in oxygenation due to a massive amount of inflammation in the lungs. By this point, viral replication is complete (see diagram 1 below). All antivirals depend on some form of viral replication to be effective. If there isn’t any, or very little viral replication, antivirals are not effective.
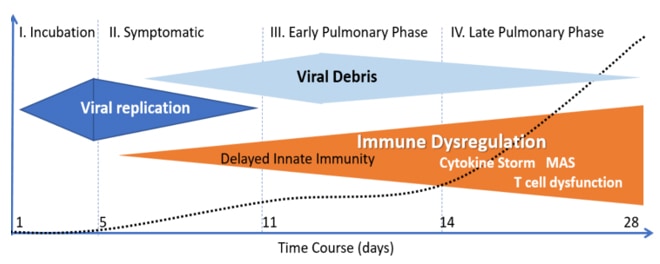
As is seen in the diagram above, by the time pulmonary symptoms are noted by patients with Covid-19, viral replication has stopped. Improvement of pulmonary symptoms due to Covid-19 was most likely due to the concomitant use of corticosteroids during the hospitalization, thereby reducing inflammation.
Besides being given too late in the disease process, another drawback to remdesivir is that it must be administered intravenously. It would be nearly impossible to administer this drug in an outpatient setting for five days in a row.
For antiviral therapy to be effective in Covid-19, it needs to be given earlier on in the disease process, before this abnormal cytokine storm, or as I like to view it, a cytokine explosion occurs. By giving antivirals early, we can contain that cytokine explosion before it can cause end organ damage (see diagram 2 below).
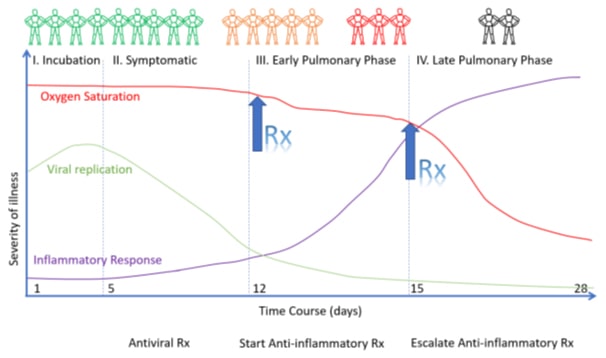
As can be seen, antiviral therapy is more effective when used while viral replication is occurring, once the patient begins to be symptomatic very early in the disease process. There are many drugs out there that can be effective in minimizing viral replication so that the cytokine explosion doesn’t occur. As discussed in my article “Covid-19 and HIV” several of my HIV patients had minimal symptoms with Covid-19, most likely due to decreased viral replication associated with their HIV medications. As a matter of fact, there are many medications out there that are effective against Covid-19, (see diagram 3 below).
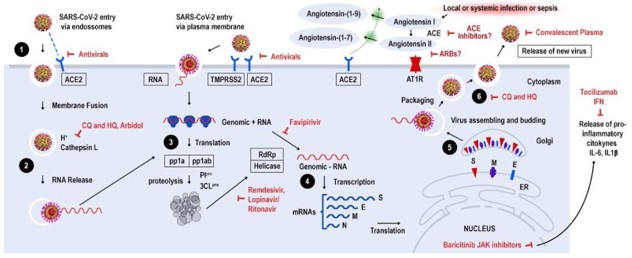
In the United States, it is well known that we are not a healthy population. Approximately 75% of our elderly population have multiple chronic conditions, or MCC’s, which means that they have more than one chronic condition. There are obesity and metabolic syndrome epidemics in this country that have exacerbated the Covid-19 pandemic. With all of these risk factors to contend with, it is necessary for us to use early therapeutics to stay ahead of Covid-19. In January of 2021, Dr. Peter McCullough, MD and colleagues published an article stratifying treatment options based on risk factors which has helped significantly in treating patients early and avoiding hospitalizations (see diagram 4 below).
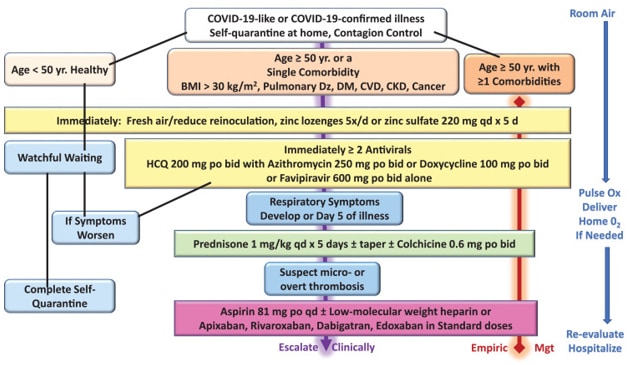
Ironically several medications contained in this flow chart are not recommended by the NIH in the treatment of Covid-19. They include doxycycline, azithromycin and hydroxychloroquine. Also not recommended in early treatment of Covid-19, is systemic steroids such as prednisone.
Favipiravir is an oral antiviral that has been used to treat viral infections such as Ebola, rabies and Lassa Fever. It inhibits RNA dependent, RNA polymerase and has been used in Russia and India. Unfortunately favipiravir has not been considered to be tested in clinical trials here in the United States for Covid-19.
Doxycycline has the ability to reduce viral replication, cellular damage and inflammation. Used in conjunction with a medrol dose pack, I am able to keep over 90% of my patients who come down with Covid-19 out of the hospital. All of these patients have MCC’s.
Azithromycin is another antibiotic with antiviral properties. It reduces the endosomal transfer of virons. It also has anti-inflammatory properties, as does hydroxychloroquine. The antimalarial drug hydroxychloroquine also has antiviral properties. Not only does it inhibit endosomal transfer of virons, but it interferes with RNA polymerase activity by helping zinc transfer intracellularly.
Prior to all the controversy involving hydroxychloroquine, I successfully used it along with azithromycin in treating patients early on in the pandemic. Again these were patients with MCC’s. Many of the studies that dismissed this combination stating that it didn’t work, was due to the fact that it was given late in the disease process. Theses medications in any number of combinations can work if given early during active viral replication.
All these drugs can be used safely, but with all medications there are adverse reactions that need to be noted and should be avoided in certain groups. It is well known that azithromycin and hydroxychloroquine together can prolong the QT interval and may trigger a dangerous arrhythmia known as torsades de pointe – it occurs less than 1% of the time. I do not use hydroxychloroquine either with or without azithromycin in patients with known heart disease, especially those with arrhythmias. Doxycycline is well tolerated, but can not be used in pregnant women and cautiously in women of child bearing years considering pregnancy.
Ivermectin is an antiparasitic macrolide with both antiviral and anti-inflammatory properties. Prior to the pandemic, I was using ivermectin for refractory chronic skin ulcers, both systemically and topically. The best work out there right now came from the American Journal of Therapeutics published in May of this year. Ivermectin appears to be beneficial for prophylaxis, early treatment, late treatment and in post Covid patients. I know clinicians who are using ivermectin in all four phases of the disease successfully and I’ve have started incorporating it my practice in battling Covid-19.
Pulmicort is an asthma inhaler that contains budesonide, a corticosteroid which some clinicians are using as an early therapeutic, with or without other adjuncts. Clinical trials are being conducted using Pulmicort. There is some concern in using inhalation therapy because it may exacerbate spread of the virus.
Supplements also play an important role, not only in combating Covid-19, but other respiratory viruses. It is amazing the number of patients I see with vitamin deficiencies. Vitamins A, C and D all have anti-inflammatory properties and Vitamin C is a powerful antioxidant. Zinc helps in decreasing viral replication. Quercetin is an immunomodulator that has been shown to have antioxidant, anti-inflammatory and antihistamine properties and is being used as an adjunct in early treatment of Covid-19. These supplements alone will not prevent Covid-19, but do help in potentially minimizing its effects and act as important support of early therapeutics.
The United States is a diverse population with many chronic conditions – a one-size fits-all approach to this pandemic has not worked, and will not work. As of August 18th, 2021, the CDC has announced that people that received the vaccine early on, are now at risk of severe disease and are urged to get a booster when eligible. We will not be able to vaccinate our way out of this pandemic because of animal resivoirs for the virus. As people struggle with this new surge, many are asking what can be done to avoid hospitalizations. Fortunately more clinicians are beginning to use early therapeutics. As this pandemic continues to evolve, we will need to have more tools in the toolbox, not less.
References for diagrams:
1) EVMS Critical Care Covid-19 Management Protocol: Paul Marik, MD https://www.evms.edu/covid-19/medical_information_resources/
2) Pathophysiological Basis and Rationale for Early OutpatientTreatment of SARS-Cov-2 (Covid-19) Infection. https://doi.org/10.1016/j.amjmed.2020.07.003