It May Not Be As Rare As We Think
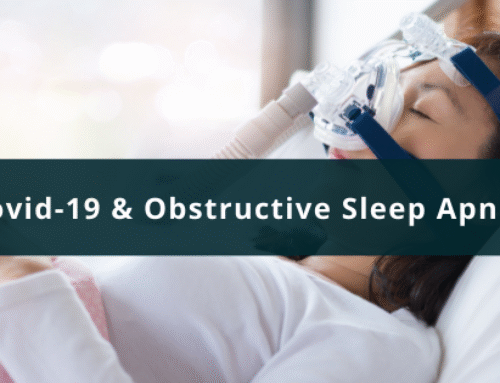
If you look at the medical literature, diabetes insipidus (DI) is a rare condition. Recently though, I have identified multiple patients with this condition. The revelation occurred, unfortunately, with the rise in symptomatic patients that are suffering with long-term consequences of Covid-19, otherwise known as ‘Long Hauler’s Syndrome’, or Post Covid-19 Syndrome. Symptoms associated with Post Covid-19 Syndrome range from losing the senses of taste and smell, a decline in executive cognitive function, also known as ‘brain fog,’ to fatigue, dizziness, and a decrease in exercise tolerance.
It must also be pointed out that there are patients who become similarly symptomatic after receiving the Covid-19 mRNA vaccine. In addition, there are many others with identical physical complaints that were suffering prior to the beginning of the Covid-19 pandemic.
It has been my belief since early in the pandemic that Covid-19 was known to create what is commonly referred to as a cytokine storm, which triggers a massive inflammatory response. The inflammatory response in severity and longevity to Covid-19 varies from patient to patient, mostly due to genetic variation. Remember, there are eight billion of us on this planet and no two are identical in every way possible.
There are other triggers that can cause this type of inflammatory response, for instance, mold exposure, zoonotic bacterial disease such as Lyme Disease, and head trauma. Regardless of the trigger, if patients develop a chronic inflammatory state, they may develop a significant amount of neuro-inflammation.
If there is enough neuro-inflammation presence in a symptomatic patient, it potentially can suppress the production of Antidiuretic Hormone (ADH), or Vasopressin. ADH is produced in the pituitary gland at the base of the brain which works by reabsorbing water in the kidneys.
This is essential to keep an adequate volume in our circulatory system to maintain a normal blood pressure. There are many moving parts to maintaining an adequate blood pressure. Two that are very important include: volume and heart rate. If your circulatory volume is low the heart rate needs to speed up to maintain a blood pressure to perfuse the organs of the body.
If there is a lack of ADH, patients lose the ability to maintain an adequate intravascular or circulatory volume. With a low intravascular volume, it becomes difficult for the body to maintain an effective blood pressure.
The most common physical findings on these patients is hypotension, low blood pressure associated with tachycardia a rapid heart rate. These findings are similarly found in patients with the diagnosis of POTS, or postural orthostatic tachycardia syndrome. The diagnosis is confirmed usually when patients have an inappropriate response to going from a laying down to a sitting up position to standing. During this movement, the patient’s blood pressure doesn’t rise in the appropriate manner and their heart rate response is too rapid. The gold standard test for POTS is the tilt table test. Unfortunately, clinicians who use to perform the test are no longer doing it or it may take months to see a provider who is preforming the test.
Symptoms associated with these patients, commonly, is dizziness and fatigue. The dizziness is easily explained because of the inability to maintain blood prefusion to the brain. This is also seen in patients with DI. Another common finding in patients with DI is polyuria, frequent urination and polydipsia, constant thirst. This makes sense. If the body has the inability to maintain an appropriate intravascular volume, the body will try and correct the problem by making you thirsty, thereby making you drink more fluids, causing the polydipsia to correct the thirst. Unfortunately, if there is a lack of ADH, then the kidneys cannot do their job by reabsorbing water into the circulatory system. If you can’t reabsorb water, the increased water intake now ends up in the bladder, causing the polyuria or an increase in making urine. Many patients who develop DI complain of frequent trips to the bathroom in the middle of the night, despite drinking more water than usual.
Fatigue is another complaint seen in patients with DI, mostly related to the rapid heart rate. Normal resting heartbeat is said to be 60-100 beats per minute for an adult. The lower your heart rate, the more efficiently your heart is pumping. More importantly is the patient’s blood pressure. In many instances, the blood pressure is low. For several patients who were very active prior to the inflammatory insult, their resting heart rates were in the 60’s to low 70’s. Now their resting heart rate is in the low 100’s. For them, a rapid resting heart rate of 100 or so, is the equivalent to them walking 24/7. This could be very fatiguing.
Another cause for the fatigue is decreased blood prefusion to the extremities to maintain an adequate blood pressure. Oxygen exchange is now compromised, making it difficult to do even low- level exercising. Frequent bathroom breaks during the night disrupt sleep, which will contribute to fatigue, too.
Making the diagnosis requires a good history to see if the patient is complaining of polyuria and polydipsia. Questions need to be asked about bouts of dizziness when they go from sitting to standing or lying down to sitting up. Have they noticed a decrease in exercise tolerance?
Laboratory tests to confirm the diagnosis include: ADH level, serum osmolality and fluid restriction osmolality. Typical findings are an undetectable ADH level and a serum osmolality either above normal, or at the high end of normal. Urine osmolarity after twelve hours of fluid restriction is usually less than 850 mOsm/kg.
Once the diagnosis is made, treatment which seems to be working well is desmopressin. Other treatment options include oxytocin and low dose naltrexone. So far, I have had success in using desmopressin.
Recently there has been a case study or two of Covid-19 causing DI. POTS is one of the more common complaints associated with post Covid-19 syndrome. It is my belief that much more work needs to be done in this field. Of course, treating the underlying cause of the chronic inflammation is most important and it can be viewed that treating the DI is just treating symptoms. I cannot disagree with that statement, but treating the DI is essential. If treating DI lessens the patient’s fatigue, they may be able to do more and work more aggressively at addressing their underlying chronic inflammatory state.
Chronic inflammation will probably be the new frontier in medicine going forward. Covid-19 unfortunately, or fortunately, depending on your view, has brought chronic inflammation to the forefront. It may help us understand the treatment for many patients, who in the past, there was no treatment for.